



























Paying to survive – the deadly toll of breast cancer in Kenya

Series Access to Medicine,
Episode 4:
In Kenya, the high price of drugs like trastuzumab, which Roche sells as Herceptin, is one reason why breast cancer is still seen as a death sentence.


When Lucia Syokau Muli found out she had breast cancer at the age of 27, no one in her community put on a pink ribbon in solidarity. In her hometown in south-eastern Kenya, cancer doesn’t trigger an outpouring of charity and support but rather fear, foreboding, and rejection.
“People think if we treat you, at the end of the day, you will die so they just neglect you and ignore you for you to take care of yourself,” Lucia, a single mother of a five-year-old girl, told SWI swissinfo.ch in front of the unmistakable purple door of the Makueni county cancer clinic, about a three-hour drive from Nairobi. “It’s like I’ve been alone on this journey.”
This is part of our series on the dilemmas facing governments, hospitals, and patients over the affordability of new, expensive treatments for cancer and other life-threatening genetic diseases. You can find all of the stories in the series on this page.
Wearing a white blouse and sporting tinted sunglasses, Lucia’s chic, confident appearance belies an agonising struggle that began when doctors found a suspicious lump in her right breast during a cancer screening. Further tests revealed that she not only had breast cancer, but an aggressive form called HER2 positive.


More
Why life-saving drugs aren’t saving lives in Kenya
“I was devastated. I even felt like slapping the doctor. I couldn’t believe it,” said Lucia, who had never met anyone with cancer. Over the last two years, she’s endured the physical and emotional stress of rounds of chemotherapy, a month of radiotherapy, and a painful mastectomy.
But just as traumatic has been the financial stress, which still hangs over her like a dark cloud. While the National Health Insurance Fund (NHIF), which requires a monthly KES500 ($4.50) contribution, covered most of her treatments, she still had to sell her beloved three-seater sofa and some other belongings to pay for diagnostic tests that aren’t covered by insurance, along with transportation and lodging for a month of treatment in Nairobi.
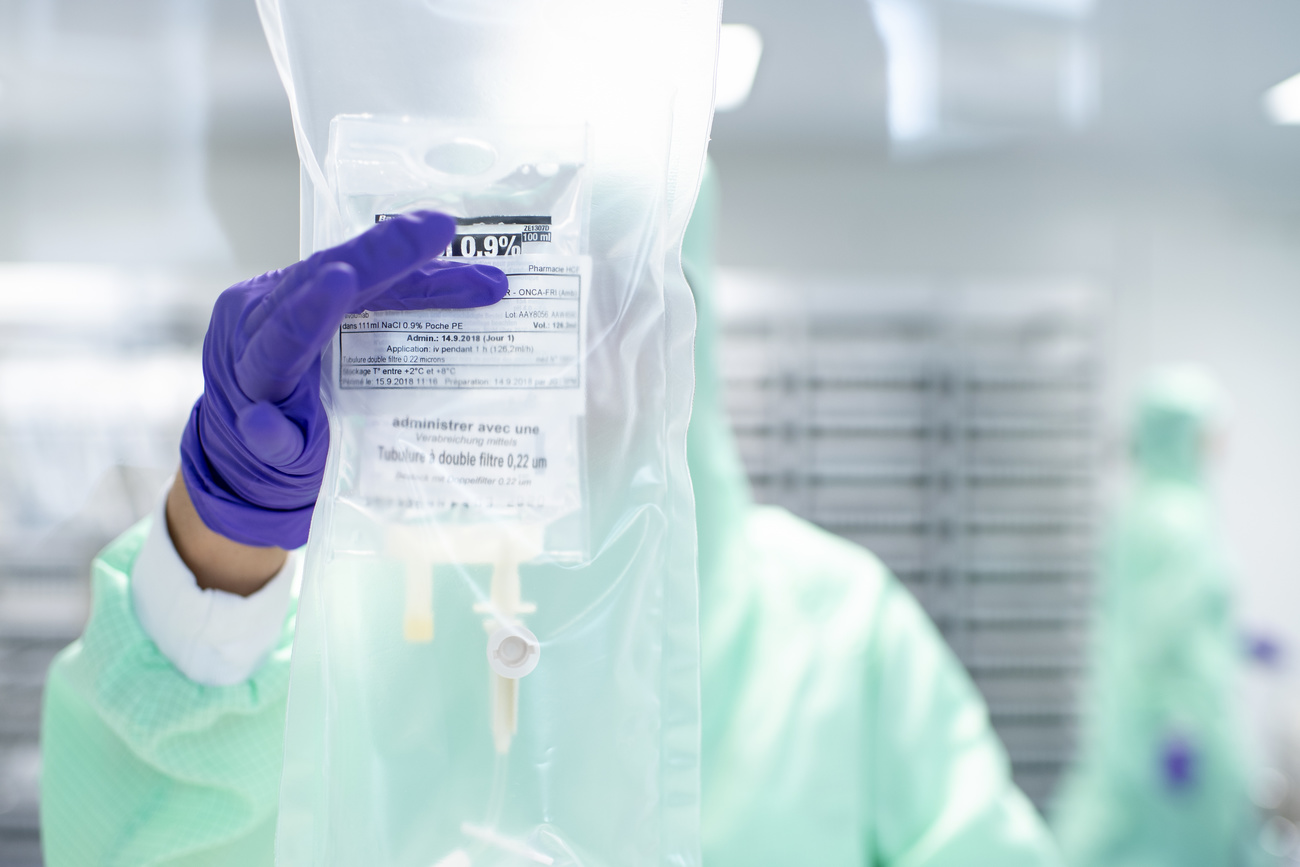
That was just the beginning. Gavin Orangi, an oncology pharmacist who runs the clinic, prescribed a targeted cancer drug called trastuzumab, a monoclonal antibody launched by Swiss firm Roche in 1998 under the name Herceptin. Approved by the US Food and Drug Administration (FDA) in 1998, it works by attacking the HER2 receptors that send growth signals to the cancer cells.
Insurance only covers four of the recommended 18 monthly intravenous injections that cost around KES70,000-120,000 (CHF600-1,100) each, nearly triple what Lucia makes in a good month selling second-hand clothes. Although her earnings are higher than the average income in Makueni, where 30% of people live below the national poverty lineExternal link of around CHF50 a month, it is way beyond her means and has left her desperate to find ways to pay for the remaining 14 cycles.
External Content
The dilemma facing Lucia is all too common across Kenya, which is confronting a rapid rise in breast cancer cases due to geneticsExternal link, lifestyle changes and improved diagnosis after years of focus on HIV and other infectious diseases. Breast cancer is now the most common cancer in Kenya with nearly 7,000 new cases per year, but with limited screening and few robust cancer registries, that’s likely an underestimate, doctors say.
Treatments like trastuzumab that dramatically improved survival for breast cancer in rich countries remain, 25 years later, still inaccessible for most women with the disease in Kenya.
Last rays of hope
Every Thursday morning, around 100 patients cram onto wooden benches, waiting for the breast cancer clinic to open at the Chandaria Cancer Centre in Eldoret, a city some 300 kilometres northwest of Nairobi. They queue for hours and sometimes overnight to see a team of cancer specialists at the centre which is part of the Moi Teaching and Referral Hospital, one of the country’s largest. The clinic, which was set up in September 2021 with support from AmpathExternal link, a partnership with several US universities, was designed to accommodate 40 patients, but it’s been bursting at the seams from demand.
Most first-time patients arrive with cancer so advanced the tumor has penetrated the skin, forming a visible wound. In many cases, the disease has spread to the bones, lungs, or spine, making it difficult to walk.
Why we chose to cover this story
There’s been incredible innovation in the treatment of cancer and other genetic diseases that is improving survival and quality of life for many people. However, these aren’t reaching most of the world. We wanted to understand why and what is being done to ensure that everyone has access to potentially life-saving treatment.
Finding sources
In all our reporting, we are vigilant in ensuring balanced reporting. This means all relevant facts and positions are considered when selecting sources to analyse a subject. In this case, we reached out to global health organisations with projects in Kenya for suggested experts, spoke to the largest pharmaceutical companies in Basel and in Kenya, and worked with a local journalist to identify government officials, hospitals, and patient organisations that are influencing the debate and create a space for patients to share their experiences. We traveled to Kenya for first-hand accounts of the topic, and to make our own observations of the issues.
If you want to know more about how we work, have a look here.
Get in touch
If you have any question regarding this topic that you’d like to have answered, or start a discussion with us and other readers, let us know via email: english@swissinfo.ch.
“It’s very rare that a patient comes with a small lump,” said Lucy Najala Wabende, a Master’s student in global health, who coordinates the clinic. One reason is that “many people don’t know the symptoms and so just ignore a lump, or they seek help from an herbalist because of their religious or cultural beliefs.” For women, the situation is often worse because they depend on their husbands for money or transport to a hospital. This all creates delays in getting a proper diagnosis.
Most worrisome is that many patients have aggressive forms of breast cancer. Wabende estimates that around 30% of patients at the clinic are HER2 positive – which means they have higher than normal levels of the HER2 protein – compared with some 20% of breast cancers globally. Some 95% of HER2 positive sufferers attending the clinic have stage IV cancer, meaning the disease has spread to other parts of the body.

More
Impressions of Makueni
For these patients, trastuzumab is one of the last remaining rays of hope. Various studiesExternal link show that the drug, in combination with chemotherapy, helps extend life for five or more years for many patients with previously untreatable breast cancer.
“Before trastuzumab, HER2 positive cancer was just bad news,” said Benjamin Anderson, a breast cancer surgeon who leads the Global Breast Cancer Initiative at the World Health Organization. “Trastuzumab turned that upside down. With it, you get outcomes that in the past were thought to be impossible.”
Trastuzumab was one of the first cancer treatments targeting the underlying cause of tumour growth to be put on the WHO Essential Medicines List in 2015, signaling it as a basic minimum for all health systems. Although newer drugs have been launched in the last decade, it is still the global standard of care for most HER2 positive breast cancers.
The long wait
When the drug was first launched “no one could touch it” because of the price said Nicholas Abinya, an oncologist at the Nairobi Hospital who has been treating cancer patients for more than 30 years. A handful of FDA-approved biosimilar drugs have come to the market since Roche’s patents on Herceptin expired a few years ago, but prices have been slow to decline. At Moi, the cost of trastuzumabExternal link is still nine times the average household income in western Kenya.
One reason is that there still isn’t enough competition, and biosimilar manufacturers are also interested to make considerable profits by targeting patients from the upper and emerging class in countries like Kenya, said Max Klein from the German NGO BUKO Pharma-Kampagne, that’s been pushing for better access to cancer drugs.
Controversy has surrounded the price of Herceptin, the brand name Roche gave trastuzumab, since the drug was launched in 1998. The Swiss company held a monopoly for years, effectively allowing it to name its price. Herceptin (trastuzumab) became one of Roche’s top three drugs in terms of revenue, generating around CHF6 billion in annual sales several years in a row.
Both South Africa and India waged a long battle with Roche to bring down the price and allow competitors to enter the market. Although the company offered lower-priced versions in those countries, the cost was still beyond what the wider public could pay.
In February this year, South Africa’s Competition CommissionExternal link recommended the company be prosecuted for “alleged excessive pricing”, arguing Roche’s pricing was “a violation of basic human rights” as it denied access to life-saving medicine for women living with breast cancer. The company has told various media that it tries to ensure the broadest access to its medicines.
Since the drug’s patent expired in Europe in 2014 and in the US in 2019, biosimilars have come to market, but problems remain. Unlike generics, biosimilars, which are copies of biological drugs are more complicated to produce and have to undergo rigorous quality tests to be approved by US and European regulators. Another challenge is the availability and cost of testing tools to determine whether someone has HER2 positive cancer.
When the WHO updated its Essential Medicines List last yearExternal link, it decided not to include new HER2 drugs because “access and affordability of trastuzumab remains very limited in resource-constrained settings”.
There are cheaper biosimilars on the market, mainly from India, but some doctors interviewed by SWI said quality and supply were inconsistent. Doctor Irene Weru who heads pharmaceutical products at Kenyatta National Hospital said they haven’t bought biosimilar trastuzumab because of quality concerns.
As around 70% of Kenyans have no form of insurance, many breast cancer sufferers don’t even begin treatment because they can’t afford it. Then there are those like Lucia, who only complete the cycles covered by their insurance. A surveyExternal link of the clinic’s patients by Wabende and her colleagues found that only 33% with HER2 positive breast cancer completed all 18 cycles of trastuzumab in 2020. Of those, only half followed the recommended dosing schedule.
“Once patients have exhausted their insurance coverage, we usually don’t see them again,” Naftali Busakhala, a physician who led the establishment of the cancer centre at Moi nearly a decade ago, told SWI. “Based on modeling studies, most of those patients die.” Many try to fundraise, asking friends and family for money, but that’s not sustainable, he said.
The high price is one of the reasons why, throughout Kenya, cancer has gained a reputation as the quickest way to poverty, and why patients face so much stigma and rejection from their communities say doctors.

More
The end of affordable medicine
While SWI was in Kenya in June, Roche signed a five-year agreement with the health ministry to provide Herceptin (trastuzumab) at a price the NHIF says will allow it to cover the full 18 cycles of treatment. Neither Roche nor the health ministry disclosed the price, but doctors suggested it is below KES60,000 (CHF500), slightly below the market rate.

The deal is for a sub-cutaneous formulation that can be administered as a five-minute injection rather than a four- to five-hour infusion, saving time and money. There are no biosimilar manufacturers to compete on the price. Four months later, talks on implementation are still underway, say doctors.
Life-or-death decisions
Kenya’s situation isn’t unique, says Anderson from the WHO. “Failure to complete treatment because of cost is the number one problem we see in low- and middle-income countries. That’s the worst of all worlds: patients get the side effects without the clinical benefit.”
This leaves doctors with agonising life-or-death decisions: they know there is a lifesaving treatment but paying for it will plunge the patient into poverty.
“When insurance only pays for four treatment cycles, what are you supposed to do?” said oncologist Jackline Majuma Makokha, who works at a hospital in western Kenya. “It’s a moral dilemma and it’s heartbreaking for us as doctors.”
Some clinics like Makueni are benefiting from a discounted price for the original HerceptinExternal link negotiated with Roche and the International Cancer Institute, a Kenyan non-profit cancer research organisation. But after insurance coverage is exhausted, the drug still needs to be paid for by patients themselves.
Gavin Orangi, Lucia’s doctor, scours the country for special deals with pharmaceutical companies who offer cheaper versions of drugs. “It is my job, it’s my prerogative to make sure that this drug is available to my patients.” Orangi adds that the high price creates problems with availability because smaller clinics like the one in Makueni with limited budgets can only purchase a few cycles at a time until they get reimbursed by insurance or patients.
Lucia was able to convince a friend to let her pose as his wife to secure another four cycles of Herceptin (trastuzumab). Then came months of waiting until the next insurance cycle, which started in August. But after two cycles of treatment, she was told the Makueni clinic had run out of the drug and she would have to postpone her next infusion. While Lucia is doing well, it’s unclear what these treatment interruptions mean for her outcomes.
Despite the uncertainty surrounding her treatment, Lucia is determined to change the widely held belief that cancer is a death sentence. She is one of the founders of a psychosocial support group for people she describes as “cancer warriors” in her community. “In the beginning, there were no medications for cancer,” she told SWI. “But now, we can say there are medications and people are being treated and they are getting well. This thing is real, and it is curable.”
Additional reporting by Mercy Murugi, a film producer in Kenya. Photo editing by Helen James. Edited by Nerys Avery.

More
Why Switzerland is among the ten fastest-warming countries in the world

More
In Switzerland four out of ten people have a migrant background – who are they?

More
Suicides in Switzerland quadruple among older people

More
French gangs target luxury cars in Switzerland

More
Renewed controversy in Switzerland over US fighter jets – explained




In compliance with the JTI standards
More: SWI swissinfo.ch certified by the Journalism Trust Initiative





You can find an overview of ongoing debates with our journalists here . Please join us!
If you want to start a conversation about a topic raised in this article or want to report factual errors, email us at english@swissinfo.ch.